

I. Introduction
II. Group Home and Green Care Farm
III. Method
1. Settings
2. Participants
3. Measurement
4. Data collection and analysis
5. Ethical considerations
III. Results
IV. Discussion and Conclusion
I. Introduction
The specific symptoms of dementia are memory loss, a reduction in practical ability, and disorientation in time and place. The decline in multiple cognitive and functional domains makes older adults with dementia more vulnerable to the influence of their surrounding environment. Consequently, the physical environment in which older adults with dementia should be thoughtfully designed to accommodate their conditions and characteristics including psychological, cognitive, behavioral, and social needs (Socialstyrelsen, 2000; Dilani, 2006; Morelli, 2006; Rahman, 2017; Nightingale, 2019; Fleming et al., 2020; de Boer et al., 2021; Lee et al., 2024; Charras, 2025). Historically, dementia care homes have predominantly followed a management-centered, hospital-like model. However, due to the negative outcomes associated with such environments⏤such as increased depressive symptoms and behavioral disturbances (Beerens et al., 2014; Migeul et al., 2016; de Boer et al., 2017; Lee et al., 2021a)⏤, alternative approaches, including resident-centered small group homes and green care farms, have gradually emerged. The development of small group home models can be traced to the pioneering efforts of Beck-Friis (1988) in Sweden. She found that transitioning dementia patients from institutional settings to a small-scale homelike setting can reduce aggressive behaviors and the use of psychotropic medications, including sleeping pills. While several studies (Davis et al., 2009; Lee et al., 2021a) have reported positive outcomes associated with small-scale group homes, Verbeek et al. (2010) found no significant differences when compared to institutional settings. More recently, the Green Care Farms (GCFs) model-an approach that integrates agriculture with care practices- has emerged as an alternative aimed at promoting independence and social participation among older adults with dementia for as long as possible (de Boer et al., 2021). GCFs enhance the resident’s well-being, offering a more stimulating and person-centered care compared to traditional facilities (Haugan et al., 2006; de Bruin et al., 2010; de Boer et al., 2015).
Although numerous studies have investigated the influence of the care environment on the quality of life (QoL) of older adults with dementia, there remains a lack of evidence-based research specifically addressing the QoL of residents with dementia in care facilities. Considering that this population is particularly vulnerable to environmental factors, there is a need for in-depth, long-term panel approach grounded in evidence-based research, rather than relying on a cross-sectional design. In this context, the present study adopts a long-term panel approach to compare the effects of different physical environments, specifically a green care farm facility and a group home care facility, on the QoL of residents with dementia. Through repeated observations over time, this comparative research seeks to examine how distinct environmental settings influence residents’ behaviors and QoL.
II. Group Home and Green Care Farm
The term of ‘group home’ combines the word ‘group’, referring to a small number of people, and ‘home’, meaning a house or residence. It refers to a small-scale, community-based residential care facility designed for older adults, particularly individuals with dementia. Group homes for older adults with dementia generally offer three key benefits: (i) a homelike, small-scale setting that is directly and indirectly associated with psychological comfort, the provision of person-centered care, and the development of trust and interpersonal relationships; (ii) convenient access for family members due to the facility’s location within the community; and (iii) enhanced job satisfaction among care aides, who work in close proximity to residents (Beck-Friis, 1988; Socialstyrelsen, 2000; An, 2014; Lee et al., 2021b). In Japan, group homes for older adults with dementia were first introduced in 1997 (Kim et al., 2008) and became firmly established during the 2000s. In Korea, influenced by cases in Japan, group homes for older adults with dementia were newly established as a type of elderly medical welfare facility following the revision of the Elderly Welfare Act in 2008 (Ministry of Health & Welfare, 2008). Guidelines specify that each unit should accommodate 5 to 9 residents with dementia, with provisions aimed at ensuring the QoL of the living environment, preventing safety incidents, and enhancing security through the implementation of locking devices. Several studies of group homes in Korea (Kim & An, 2008; Kim, Jung, & Kim, 2008; An, 2014; Nam, 2018) have found that these facilities tend to provide more shared rooms for 3-4 residents than single private rooms, and that they offer an institutional atmosphere rather than a homelike one. There is a need for study to assess whether group homes for older adults with dementia are effectively managed to fulfill their ultimate goal of improving residents’ QoL.
As an alternative to traditional institutional care, a green care farm is a care facility that integrates agricultural activities and natural environments with social and health services to promote physical, emotional, and social well-being among vulnerable population (Hassink et al., 2020). GCFs have emerged as a form of innovative care environment and are increasingly expanding across various contexts in European societies, including social and therapeutic horticulture, animal-assisted therapy, and care farming (Berget et al., 2010; de Boer et al., 2017). There are diverse domains under the broader umbrella of ‘green care’ (See <Figure 1>).
Green care encompasses a range of activities that promote physical and mental health and well-being through contact with nature (Berget et al., 2010; Haugan, 2006). In the Netherlands, one of the leading countries in GCFs, there are over 1,000 green care farms. Recently, some of these farms have been established to provide 24-hour care (Verbeek, de Boer, & Hamers, 2014). The philosophy behind GCFs is that people are encouraged to participate in daily activities, and the physical environment offers many opportunities to incorporate activities of normal daily life (de Boer et al., 2017). Residents of green care farms have the opportunity to engage in a variety of daily activities, including outdoor, indoor, and work-related activities. According to the study by de Boer and his colleagues (2017), residents of GCFs are more frequently engaged, experience more social interaction, and spent more time outdoors during the day compared to those in traditional nursing homes.
Examining the behaviors and QoL of older adults with dementia in group homes and GCFs⏤which are established as alternatives to traditional institutional care environments⏤may provide meaningful insights. Since the two groups consist of older adults with dementia from two countries with differing cultural backgrounds, it is presumed that the observed behavioral differences may be influenced not only by physical environmental factors but also by cultural elements. Nevertheless, both groups share a significant commonality in that they are affected by dementia, are unable to live independently at home without support, and reside in care facilities where they receive 24-hour supervision and support. Therefore, it is deemed appropriate to compare them as subjects of study. Such a comparative analysis is considered meaningful in exploring the future direction of domestic group home care.
The operational definitions of the group home and green care home facilities are as follows: (i) A group home is a small-scale residential facility where five to nine older adults with dementia live together and receive 24-hour personal care in a homelike setting. (ii) A green care farm is a residential dementia care facility that provides 24-hour accommodation and care services within a farm-based setting.
III. Method
This study presents the quantitative data regarding the role of the built environment on the behavior and QoL among the residents with dementia in Seoul, South Korea, and in Laarbeek, the Netherlands. Given that the study subjects are vulnerable to their surrounding environment, behavioral observations were conducted in three sessions over the course of one year to avoid temporal bias and obtain a consistency of data.
1. Settings
To select care homes appropriate for the study purpose in Seoul, a list of 25 dementia care homes was compiled based on data reported by the Seoul Metropolitan Government. The primary investigator contacted the managers of each care home and conducted site visits to eight care homes, obtaining study cooperation from two of them. This paper analyzes and compares data from a care home, Han-River, which was selected as the appropriate subject to a counterpart⏤a green care farm in the Netherlands. Group home Han-River is a small-scale facility with nine residents with dementia in a unit.
The Wageningen Care Farm Institute was commissioned to contact green care farms in the Netherlands that provide residential facilities and 24-hour care services, and subsequently inquire about their willingness to participate in the study. Two green care farms agreed to participate in focus group interviews with staff, and one of them was unable to participate in the observation study due to internal circumstances. Therefore, the green care farm Golden Tulip, located in Laarbeek, participated in the observational study. It has six independent houses with four to eight older adults with dementia living in each house and two daycare centers.
2. Participants
The study participants were older adults with dementia living in a dementia care facility. Residents were selected based on the following criteria in accordance with the purpose of the study: aged 60 years or older, had resided in the facility for more than one month, and were able to walk either independently or with the use of an assistive device. Residents who were bedridden or remained in their private rooms during the daytime were not included, as observations were conducted exclusively in public areas of the facility. By defining the above-mentioned criteria, including age, minimum stay, and physical functioning, the study sought to minimize cognitive and behavioral differences between the two groups. Five residents from the Han-River group home participated in the observational study. At the green care farm Golden Tulip, seven residents initially met the study criteria. However, three residents either relocated or passed away; therefore, data from a total of four residents were included in the final analysis.
To ensure anonymity and confidentiality, the names of the care homes in the paper were assigned pseudonyms.
3. Measurement
1) Physical environmental characteristics of the participating care homes was assessed using the Therapeutic Environment Screening Survey for Nursing Homes (TESS-NH) tool (Sloane et al., 2002). The TESS-NH designed to evaluate the physical and psychosocial environmental characteristics of nursing homes in terms of the therapeutic potential for residents with dementia. This tool is composed of six domains, with a total of 84 individual items that assess specific aspects of the environment, using a standardized checklist format. The six domains are: i) privacy/control/autonomy: unit autonomy, access to outdoors and privacy; ii) safety/ security/health: exit control, maintenance, cleanliness and safety; iii) stimulation: lighting, visual/tactile stimulation and noise; iv) socialization: space and seating; v) personalization/homelikeness: familiarity and homelike features, and vi) orientation: orientation and cueing. The physical features were for the most part rated on a scale from 0 (distinctly unpleasant attribute) to 3 (more favorable attribute). It was conducted by a principal investigator, who visited dementia care facilities in person and assessed each space based on the evaluation items through direct observation of the site.
2) The behaviors of the residents were measured using the Dementia Care Mapping (DCM) tool. DCM is a structured, observational framework developed by the Bradford Dementia Group, University of Bradford that is used to evaluate the QoL and quality of care for the perspective of residents with dementia (University of Bradford, 2010). The tool provides insight into how environmental and interpersonal factors affect behaviors and QoL of individuals with dementia. Behavioral Category Codes (BCCs) are a set of standardized behavioral codes in the DCM framework. The BCCs consisted of 23 codes1) that categorize observable behaviors of residents with dementia. By using these behavioral profiles, levels of potential engagement―both high and low―and withdrawal can be assessed as key determinants influencing the quality of life in residents with dementia.
(1) High Potential Engagement: It refers to the degree of potential for positive engagement with the surrounding environment. It was measured by the percentage of time spent in behaviors such as ‘interacting with others’ (code A), ‘self care’ (code D), ‘creative activities’ (code E), ‘eating and drinking’ (code F), ‘intellectual abilities’ (code I), ‘exercise’ (code J), ‘walking, standing’ (code K), ‘recreational activities’ (code L), ‘attachment to inanimate objects’ (code O), ‘direct engagement of the senses’ (code T), and ‘work or work-like activity’ (code V).
(2) Low Potential Engagement: It refers to a state where individuals with dementia exhibit minimal levels of meaningful interaction, activity participation, or engagement in their peers, caregivers, or surroundings. This is associated with behaviors ‘being disengaged, withdrawn’ (codes C), ‘attempting to communicate without receiving a response’ (code U), and ‘repetitive self-stimulation’ (code W).
(3) Withdrawal: It means that residents do not show any signs of engagement with themselves or the environment around them. It corresponds to the behavior ‘being disengaged, withdrawn’ (code C) and ‘sleeping, dozing’ (code N).
4. Data collection and analysis
The principal investigator, who was certified by Jentle Harts Consulting after completion of the DCM Learning Course, unobtrusively observed the selected residents from the group home Han-River and the green care farm Golden Tulip. Mapping was conducted at five-minute intervals, typically between 9:30 and 16:00, in public areas. To obtain rich data, observations were conducted over two to three days per unit. To ensure data reliability and minimize temporal bias, the same mapper conducted observations three times over the course of one year at each site. Observations were conducted in different years due to different research projects. At Han River, observations were carried out in April~May 2019 (T1), September 2019 (T2), and January 2020 (T3). At Golden Village, observations took place in January~February 2024 (T1), May 2024 (T2), and August 2024 (T3).
Data were coded and analyzed using Microsoft Excel Program. Descriptive statistics, the Shapiro-Wilk test, and t-test were used to compare the study groups in terms of behavioral categories and QoL with the significance level set at p < 0.05. Given the relatively small sample size, the Shapiro-Wilk test was employed to assess the normal distribution of the data, and t-test were subsequently conducted on variables that met the assumption of normal distribution.
5. Ethical considerations
This study was conducted in accordance with ethical standards for research involving human participants. Ethical approvals were obtained from the Institutional Review Board of Yonsei University.2)
The purpose of the study and the detailed observation procedures were fully explained to all participants and their families. Written informed consent was obtained prior to participation. For participants who were unable to express voluntary consent due to cognitive limitations, consent was obtained from their families or legal guardians.
III. Results
<Table 1> presents the general characteristics of the selected residents and care homes, along with the results of the t-test on the physical environmental characteristics. The data for the participants in Han-River included a total of five residents with dementia, all of whom were female, with an average age of 91.2 years. At the Golden Tulip, data from a total of four residents, including two females, were analyzed, with an average age of 86.5 years.
Table 1.
General Characteristics of the Participated Subjects and Results of t-test Analysis on Physical Environmental Characteristics


The results of t-test analysis on the physical environmental characteristics indicate statistically significant differences in the dimensions of stimulation (t19 = - 5.22, p < 0.001) and personalization/ homelikeness (t5 = - 4.21, p < 0.01), whereas no significant differences were observed in the dimensions of privacy/control/autonomy, safety/security, socialization, and orientation. This outcome demonstrated that the green care farm Golden Tulip provided a significantly more caring atmosphere in terms of lighting, stimuli and a more personalized and homelike setting compared to Han-River.
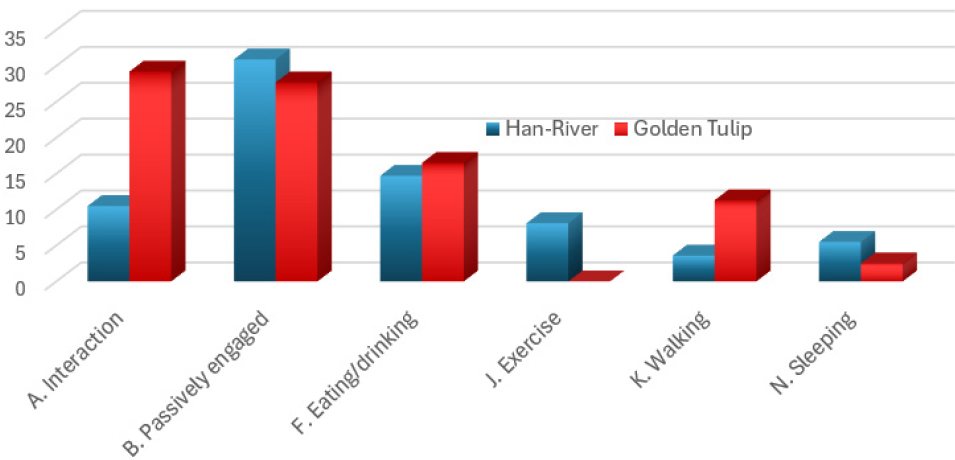
<Table 2> presents the distribution of behavioral category profiles across three observation times (T1-T3), along with the t-test results for levels of potential engagement (high/low) and withdrawn behavior. Behaviors that accounted for more than 10% or showed statistically significant differences are presented in <Figure 2>. Participants at the green care farm, Golden Village, spent approximately three times more engaging in interactions with others and walking compared to those at the group home, Han River. Meanwhile, residents at Han River spent more time engaging in structured exercise provided by the facility and more time sleeping during their remaining hours compared to their counterparts at Golden Village.
Table 2.
Distribution of Behavior Codes and Results of t- test
| Behavior Codes※ | Han-River | Golden Tulip | t-value (df) | |||||||
| mean % | (T1 | T2 | T3) | mean % | (T1 | T2 | T3) | |||
| A. Articulation | Interaction with others | 10.5 | (10.2 | 12.1 | 9.2) | 29.2 | (21.4 | 36.7 | 32.2) | t(2) = - 5.21* |
| B. Borderline | Being engaged but passively (watching) | 30.9 | (29.4 | 32.9 | 30.4) | 27.7 | (39.3 | 14.4 | 25.0) | N.S. |
| C. Cool | Being disengaged, withdrawn | 1.4 | (1.8 | 2.3 | 0.0) | 0.0 | (0.0 | 0.0 | 0.0) | N.S. |
| D. Doing for self | Self-care | 4.5 | (5.8 | 3.0 | 4.6) | 1.4 | (0.5 | 1.7 | 2.2) | N.S. |
| E. Expressive | Expressive or creative activities | 0.3 | (1.0 | 0.0 | 0.0) | 0.9 | (0.9 | 0.5 | 1.4) | N.S. |
| F. Food | Eating/ drinking | 14.7 | (12.6 | 14.6 | 17.1) | 16.5 | (15.4 | 15.9 | 18.1) | N.S. |
| I. Intellectual | Prioritizing the use of intellectual abilities | 0.7 | (0.6 | 1.5 | 0.0) | 0.7 | (1.2 | 0.3 | 0.6) | N.S. |
| J. Joints | Exercise or physical sport | 8.1 | (6.0 | 9.8 | 8.4) | 0.0 | (0.0 | 0.0 | 0.0) | t(2) = 7.27* |
| K. Come & go | Walking, standing or moving activities | 3.6 | (4.4 | 2.0 | 4.3) | 11.3 | (13.9 | 10.4 | 8.9) | t(2) = - 4.81* |
| L. Leisure | Leisure, fun and recreational activities | 6.2 | (7.6 | 1.8 | 9.2) | 2.4 | (1.4 | 5.7 | 1.0) | N.S. |
| N. Nod | Sleeping, dozing | 5.5 | (6.2 | 3.5 | 6.8) | 2.5 | (2.2 | 3.0 | 2.4) | N.S. |
| O. Objects | Displaying attachment to inanimate objects | 3.4 | (2.8 | 7.3 | 0.0) | 0.1 | (0.0 | 0.0 | 0.2) | N.S. |
| P. Physical | Receiving practical or personal care | 3.7 | (3.4 | 3.0 | 4.6) | 0.5 | (1.4 | 0.0 | 0.0) | N.S. |
| T. Timalation | Direct engagement of the senses | 0.1 | (0.0 | 0.3 | 0.0) | 1.8 | (1.4 | 3.7 | 0.8) | N.S. |
| U. Unresponded to | Communicating without receiving a response | 0.1 | (0.0 | 0.0 | 0.3) | 0.0 | (0.0 | 0.0 | 0.0) | N.S. |
| V. Vocational | Work or work-like activity | 0.4 | (0.4 | 0.5 | 0.3) | 2.6 | (0.3 | 4.2 | 3.8) | N.S. |
| W. Withstanding | Repetitive self-stimulation | 1.1 | (2.4 | 0.5 | 0.3) | 0.0 | (0.0 | 0.0 | 0.0) | N.S. |
| X. X-cretion | Episodes related to excretion | 5.0 | (5.4 | 5.0 | 4.6) | 2.4 | (0.7 | 3.5 | 3.4) | N.S. |
| Total | 100.0 | (100.0 | 100.0 | 100.0) | 100,0 | (100,0 | 100,0 | 100,0) | ||
|
High Potential Engagement (corresponds to behavior category A,D,E,F,I,J,K,L,O,T, and V) |
mean (SD) 4.77 (4.90) |
6.21 (9.47) | N.S. | |||||||
| Low Potential Engagement (corresponds to behavior category C, U and W) |
mean (SD) 0.84 (1.02) |
0.0 (0.0) | t(8) = - 2.49* | |||||||
| Withdrawn Behavior (corresponds to behavior category C and N) |
mean (SD) 3.43 (2.64) |
1.27 (1.41) | t(5) = - 2.97* | |||||||
The t-test results of the behavioral categories demonstrated that the residents of the Golden Tulip exhibited significantly higher levels of interaction with both neighbors and staff, as well as more engagement in walking and mobility activities, compared to those of the Han-River (t2 = - 5.21, p < 0.05 and t2 = -4.81, p < 0.05 respectively). Conversely, those of the Han-River engaged in significantly more structured physical exercise than their counterparts (t2 = 7.27, p < 0.05). Regarding high potential engagement, an indicator of positive engagement in a care environment, there was no significant difference between the two groups. However, there were statistically significant differences in low potential engagement and the withdrawn behavior (t8 = - 2.49, p < 0.05 and t5 = - 2.97, p < 0.05 respectively) between the groups. Although the standard deviations of these behaviors were relatively large, indicating behavioral instability among the participants, the significant differences observed remain noteworthy. These results suggest that residents in Han-River exhibited minimal interaction with their neighbors, limited participation in activities, and a general indifference toward engaging with their surroundings compared to those of Golden Tulip.
IV. Discussion and Conclusion
This observational study compared the behavior and QoL of residents with dementia living in a group home and a green care farm, with variations in the surrounding environments in Seoul, Korea and in Laarbeek, the Netherlands.
The QoL of the residents was assessed using the DCM tool on three occasions over the course of one year. The results showed that residents with dementia living on the green care farm are likely to interact with both neighbors and staff, and spend more time engaging in physical activities such as walking or exploring the outdoor environment. These findings may be attributed to the supportive setting of a green care farm, which
offers positive stimuli and fosters a homelike atmosphere. Furthermore, these results align with the findings of Steinmann, Hamers, and Verbeek (2025), who reported that green care farms stimulate engagement in activities that help retain physical functioning, while also enabling residents to enjoy freedoms and autonomy. In addition, staff members in Golden Tulip naturally encouraged residents with dementia to participate in daily tasks such as meal preparation and clean up after meals. For instance, it was common to observe both residents and staff peeling potatoes or cutting vegetables together in preparation for lunch. These lifestyle activities including domestic, outdoor, and social activities contribute positively to maintaining residents’ sense of identity and further supports the preservation of their remaining cognitive and motor abilities (Cohen-Mansfield, Golander, & Arnheim, 2000; Surr, 2006; Cipriani et al., 2020; Verbeek et al., 2025). In line with this, Davis and her colleagues (2009) argued that the built environment must effectively support residents’ basic everyday living experiences to ensure they receive adequate care. Similarly, several studies (Bengtsson & Carlsson, 2006; Haugan et al., 2006; Lee, Chaudhury, & Hung, 2016) asserted that a well-designed outdoor environment could help residents release frustration and temporarily escape negative conditions, while also providing opportunities for enjoyment and reminiscence. Building on these findings, green care farms with a homelike atmosphere⏤where daily activities such as walking, raising livestock, and growing vegetables are readily accessible⏤can be regarded as environments that enhance residents’ sense of identity and overall well-being. However, as Haugan and her colleagues (2006) emphasized, it is essential that green care farms be well-maintained in order to function effectively as a supportive residential environment for older adults with dementia. This includes ensuring the quality of buildings, implementing risk and hazard management strategies, minimizing noise, and ensuring overall safety.
On the other hand, residents of the Han-River group home primarily engaged in structured physical exercise programs, in contrast to those in the other cohort. This difference may be attributed to the limited availability of outdoor space, which restricts opportunities for safe and comfortable outdoor activities such as walking or enjoying fresh air and sunlight. Indeed, care homes located in metropolitan areas often face such spatial constraints. Therefore, it is necessary to consider and implement alternative solutions⏤such as the development of rooftop gardens⏤ to enhance residents’ access to outdoor environment in urban settings. Furthermore, according to the results of the t-test, residents in this group demonstrated relatively passive behavior, showing limited responsiveness to stimuli and increased tendencies toward social withdrawal. From an environmental perspective, although a dementia group home operates under a small group home model, the lack of a supportive indoor and outdoor environment, which is characterized by a dull and institutional atmosphere, appears to be a contributing factor to these negative outcomes. The findings are in line with previous studies (Lee et al., 2021; Brennan & Doan, 2023), which found that residents’ well-being was lower in non-supportive dementia care settings. Meanwhile, the factor of the care philosophy, which was not included in this study, may also be directly associated with the behavior of the residents with dementia.
This study has limitations that should be acknowledged. First, the analysis was conducted with a relatively small number of facilities and participants. Given these limitations, the generalizability of the findings to the broader dementia population and other dementia care facilities is restricted. Moreover, since the results may have been influenced by specific individual characteristics⏤such as participants’ health status, cognitive level, and social background⏤it is challenging to directly apply the findings to other cohorts. To address these limitations, future studies should aim to include a more diverse range of care facilities and more representative sample of participants, taking into consideration factors such as dementia severity and major life events. Second, the study did not included participants’ levels of engagement⏤such as the degree of participation, or emotional involvement⏤. A more comprehensive analysis on engagement levels could have added further depth to the findings. Despite these limitations, the significance and value of the repeated behavioral observation data remain substantial.
This study supports that a physical environment with a homelike atmosphere and appropriate outdoor areas is directly or indirectly associated with the behavior and QoL of older adults with dementia. Future studies are needed to examine the factors underlying the care philosophy of facilities to obtain more detailed and accurate data, as these are associated with the QoL of the residents. The care philosophy may influence aspects such as control and autonomy, dependence and independence, and the relationship between caregivers and care recipients, all of which are closely related to the residents’ quality of life.
